|

Breast Cancer
Epidemiology
Risk Factors
Diagnosis
History
Physical Examination
Breast Imaging
Mammography
Ultrasound
MRI
Biopsy
Systemic Evaluation
Pathology
Normal breast anatomy
Lobular
Carcinoma in situ (LCIS)
Ductal Carcinoma in situ (DCIS)
Invasive Breast Cancer
Receptors Status
Grading
Breast Cancer Staging
Molecular characterization
Oncotype
DX
Mammaprint
Spread
Therapy
Lobular
Carcinoma in situ (LCIS)
Ductal Carcinoma in situ
(DCIS)
Invasive
Cancer
Surgery
Radiation therapy
Drugs
therapy
Chemotherapy
Hormonal therapy
Biologic therapies
References
Breast cancer is the most
prevalent malignancy and the second cause of cancer related
death among women (1). According to the World Health
Organization's (WHO) World Cancer Report, 2003, more than
one million new cases of breast cancer are diagnosed
worldwide each year (2, 3). In 2009, about 192,370 women are
estimated to be diagnosed with breast cancer (1), and more
than 40,000 patients are expected to die from this disease
in the USA (1). In Arab countries, population-based
screening is not a common practice; locally advanced disease
accounts for higher percentage of the newly diagnosed breast
cancers there (4, 5).
The causes of breast cancer in
the majority of patients remain undetected. Risk factors for
this malignancy include:
-
Patient’s sex.
Breast cancer is much more
prevalent among females than among males. The estimated
number of new cases of breast cancer in the USA during
the year 2009 is about 192,370 women, versus 1910 men
(1).
-
Age.
There is increase in the incidence of breast cancer with
increasing age (6). Breast cancer is the leading cause
of cancer related death among women between the ages of
20-59 years (1).
-
Family history
and genetic factors.
Genetic factors play an important role in breast cancer.
The risk for a woman to develop breast cancer is 1.5 to
3 times higher if she has a sister or a mother who
suffer from breast cancer (6). Mutations in some genes
were found to result in increased risk for breast
cancer. Mutations in Breast Cancer Associated Gene 1 & 2
(BRCA1, BRCA2) results in increased incidence of breast
and ovarian cancer. These mutations are associated with
breast cancer in young women.
-
Menstrual
cycle. Breast cancer risk
increase with the number of menstrual cycles that the
woman experiences during her life. Late menarche, early
menopause, and pregnancy are associated with less
menstrual cycles and thus a lower risk for breast
cancer.
-
Breast feeding.
Women who breastfeed their children seems to have less
breast cancer. The odds ratios for breast cancer are
lower with increasing duration of breastfeeding (7).
-
Obesity.
Obesity is a risk factor for breast cancer (6, 8, 9).
Increased physical activity is associated with lower
risk for breast cancer (9).
-
Radiation.
Previous radiation therapy
to chest wall increases the risk for breast cancer.
History.
Taking history from the patient is very important for the
diagnosis of any breast pathology. The main questions for
the patient are:
1.
Is there any
lump in the breast, in the underarm area, or in the neck
region?
2.
Did the
patient note any new asymmetry in the breasts?
3.
Is there a
retraction of the nipple?
4.
Is there any
change in the texture of the breast skin? Any ulceration of
the breast skin?
5.
Is there a
history of cancer for the patient or his relatives?
Physical
Examination. Inspection.
Physical examination starts with inspection of both breasts.
The physician pays special attention to any lumps or
irregularities in the breast structure, and to the skin
texture of the breast. Early stages of breast cancer are
usually unnoticed by inspection. Centrally located breast
tumors may result in retraction of the nipple. Breast cancer
infiltrating the skin may results in change of the skin
texture of the affected breast. Advanced breast cancer with
ulceration of the skin can be easily seen by inspection.
Palpation. Palpation of the breast and its lymph
node draining areas (underarm, above and below the clavicle,
and the area beside the sternum) is pivotal for the
diagnosis and evaluation of breast cancer. Systematic
approach for breast examination is employed by most
oncologists, with special attention for areas indicated by
the patient, suspected by inspection, or specified in
previous imaging procedures that the patient already
performed.
Breast Imaging
Mammography. Mammography is
used both for screening and diagnosis of suspicious lesions
of the breasts.
Ultrasound.
Ultrasound is used
to further define any suspicious lesion discovered
either by physical examination or mammography. Ultrasound is
also utilized to guide core needle biopsy or fine needle
aspiration (FNA).
MRI.
The role of MRI in diagnosis
and management of primary breast cancer is not clear-cut.
MRI may be important in young women with dense breast tissue
(which usually is difficult to evaluate by mammography),
other clinical scenarios in which MRI may be of benefit are
cases in which there is an enlarged lymph node in the
underarm with proved biopsy of breast cancer, but all other
studies (physical examination, mammography and ultrasound)
do not show where the primary tumor is. In such situations
MRI may give the answer. MRI can also be used to follow
young healthy women with proved genetic mutation in BRCA1 or
BRCA2 genes, in order to detect any malignancy at an early
stage.
Biopsy.
Tumor biopsy is critical for
the diagnosis of breast cancer, and to discriminate it from
other non-malignant lesions. For large palpable lesions,
biopsy can be performed without the guidance of imaging. For
impalpable lesions, the biopsy is usually performed under
the guidance of an imaging modality (mammography/
ultrasound). Fine Needle Aspiration (FNA) or Tru-cut biopsy
(thicker needle that cuts part of the lesion) is usually
used to obtain tissue from the suspicious mass. Once
material from the tumor is obtained, pathological evaluation
under microscope can be performed. If an enlarged lymph node
is detected in the axilla (underarm), additional biopsy
should be obtained from it as well.
Systemic Evaluation.
Systemic evaluation is a work up that is done to test if
cancer has spread outside the breast or its regional lymph
nodes. Systemic evaluation is performed to answer the
question: Have this breast cancer send metastasis? Stage I
breast cancer (node negative breast cancer and tumors less
than 2 c"m) rarely send metastasis at time of diagnosis and
systemic evaluation is not usually necessary. For node
positive breast cancer and tumors larger than 2 c"m systemic
evaluation should be considered. Systemic evaluation usually
includes bone scan (to exclude bone metastasis), CT scan of
the chest, and abdominal CT or ultrasound.
Normal
breast anatomy. Breast tissue
contains glands (mammary glands which are responsible to
milk production after child delivery). These glands end in
lactiferous ducts that drain into pores in the nipple.
Lobular
Carcinoma in situ (LCIS).
LCIS is a premalignant lesion. Women
with LCIS are at higher risk to develop breast cancer in the
same breast in which the lesion was detected, as well as in
the contralateral (the other) breast. (See
treatment of LCIS
below).
Ductal Carcinoma in situ (DCIS). DCIS is
non-invasive cancer (do not send metastasis), but is a
precursor for invasive carcinoma, and thus should be
treated. Treatment of DCIS usually includes surgery±
radiation therapy. (See treatment of DCIS below).
Invasive
Breast Cancer. Invasive cancer
is a malignant disease (tumor with ability to send
metastasis). The two major pathological entities of invasive
breast cancer are: Invasive Ductal Carcinoma (IDC) and
Invasive Lobular Carcinoma (ILC). IDC have some variants
with better prognosis: A. Tubular Carcinoma, this cancer is
composed of well differentiated cells, B. Mucinous (colloid)
carcinoma- tumor cells produce a mucos/jelly-like material,
these tumors are usually well differentiated, highly express
estrogen receptor (good thing) and usually do not express
HER2 (less aggressive tumor); mucinous carcinoma is less
likely to metastasize to lymph nodes compared to other
breast cancers. C. Adenoid Cystic carcinoma of breast is
rare and has a good prognosis, with low metastatic
potential.
Receptors
Status. Each malignant breast
tissue, obtained either through breast biopsy or operation
(partial or total breast excision), should be evaluated for
the expression of:
A.
Estrogen
Receptor (ER).
B.
Progesterone
Receptor (PR).
C.
Human
Epidermal growth factor Receptor 2 (HER2).
The evaluation of the receptors
status is determined by a method called immunohistochemistry.
The results range from 0 to +3. For ER and PR the percent of
tumor cells stained for the specific receptor is evaluated
as well. For HER2, results of 0 or +1 are regarded as
negative, results of +3 as positive, and +2 as inconclusive.
If the result is +2 a more specific study should be
performed, this study is called "FISH" (Fluorescence in Situ
hybridization).
Grading
Grading of breast cancer relies
on the pathological appearance of the tumors cells. There
are three grades:
Grade 1: Low grade = well
differentiated cells (good prognosis).
Grade 2: Intermediate grade.
Grade 3: High grade= poorly
differentiated cells (highly malignant).
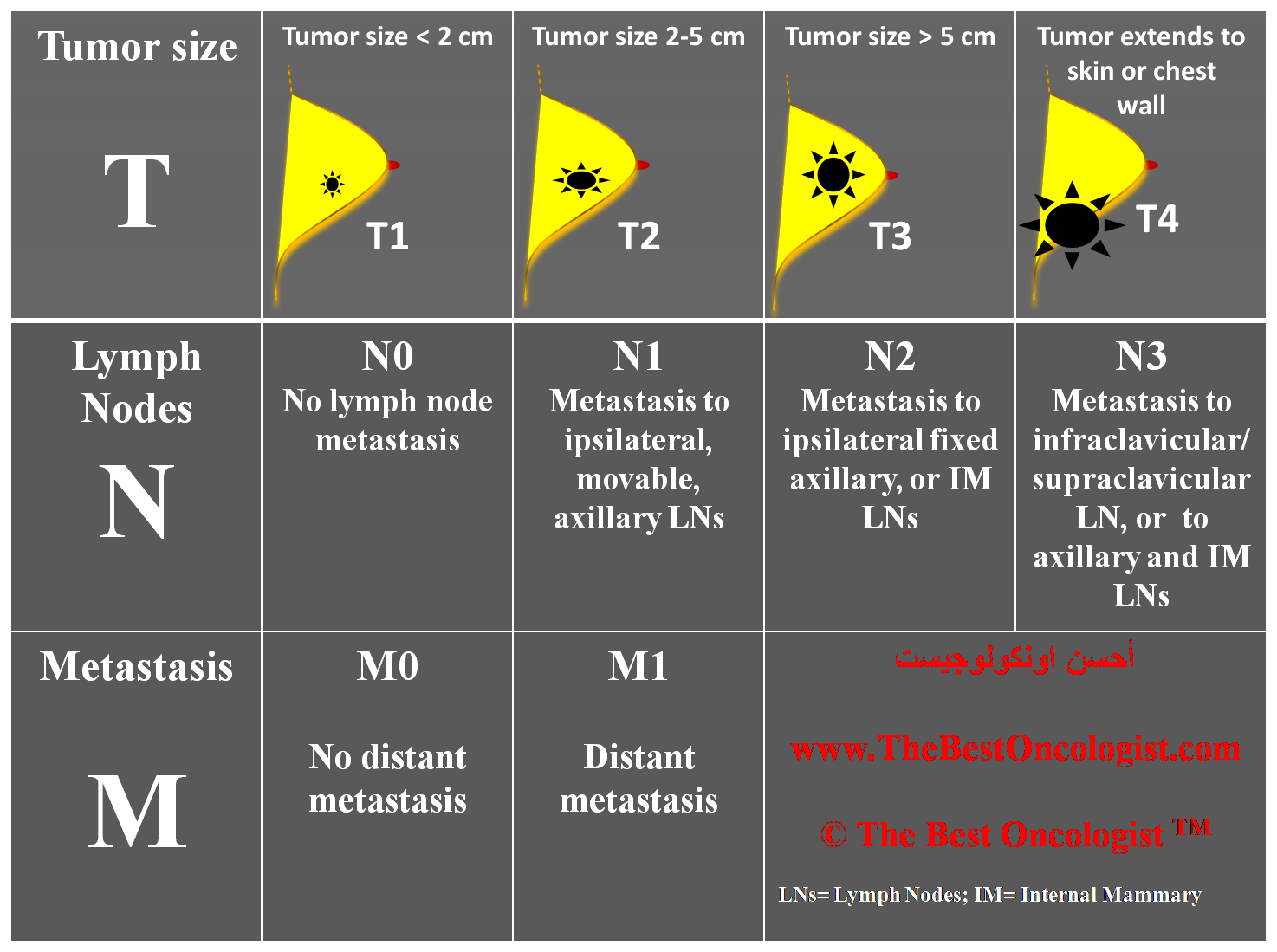
Breast cancer is classified
according to the TNM staging system suggested by the
American Joint Committee on Cancer (AJCC) (10). The staging
system takes into account the primary tumor characteristics
(T1-T4, see table below), lymph nodes involvement (N0-N3,
see table below), and the presence (M1) or absence (M0) of
distant metastasis. Regarding the lymph nodes involvement,
presence of tumor cells within a lymph node with a diameter
of more than 2 mm is defined as metastasis; between 0.2- 2
mm micro-metastasis; and less than 0.2 mm as isolated tumor
cells. The clinical meaning of micro-metastasis and isolated
tumor cells are not totally clear. Pathologic staging of
lymph nodes relies upon the number of involved nodes: N0 =
no lymph node involvement; N1= 1-3 lymph nodes with
metastasis; N2= 4-9 lymph nodes with metastasis; N3 ≥ 10
lymph nodes with metastasis.
TNM definitions in Breast
Cancer Staging
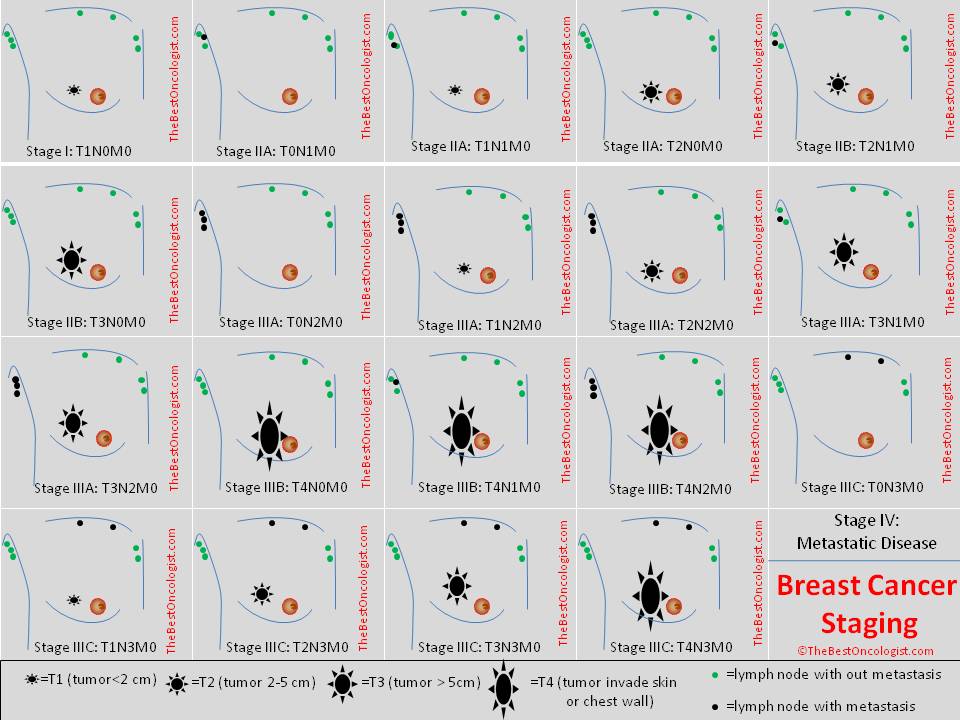
Breast Cancer Staging
Oncotype
DX. This test examines breast
tissue embedded in paraffin (after biopsy or operation, the
resected breast tissue is embedded in paraffin to facilitate
histological examination, and to preserve the tissue for
long period of time). Oncotype DX tests the RNA
levels of 21 genes. 16 of these 21 genes are related to
cancer, while the other five are reference genes tested to
calibrate the results. The test was primarily designed to
predict the likelihood of breast cancer recurrence for women
with node-negative, estrogen-receptor-positive (stage I)
invasive breast cancer treated after operation with
Tamoxifen only (11, 12). Oncotype DX assay gives a
number for each test called "Recurrence Score". The
likelihood of distant recurrence at 10 years increases
continuously with an increase in the Oncotype DX
assay Recurrence Score® result (11, 12), Oncotype
DX assay was able to stratify these patients into three main
groups: Low risk for recurrence, Intermediate risk, and High
risk. Women with low recurrence score are usually treated
with hormonal therapy only (no chemotherapy is given after
breast operation); women with high recurrence score are
usually treated with both chemotherapy and hormonal therapy;
intermediate group treatment is usually individualized.
Another study showed that Oncotype DX Recurrence
Score in women with stage I, node negative, estrogen
receptor positive breast cancer tumors, can predict which
women will benefit from chemotherapy. Women with high
recurrence score (score ≥31) had a large benefit from
chemotherapy. Patients with low recurrence score
(< 18) derived minimal, if any, benefit from
chemotherapy treatment, recurrence score of 18-31 is a gray
zone (13). Recent results show that Oncotype DX test
can predict response to chemotherapy in women with breast
cancer and 0-3 positive axillary lymph nodes (14).
Mammaprint.
Mammaprint test the expression of RNA of a set of 70 genes
related to breast cancer by microarrays method (15, 16). The
test utilizes fresh frozen breast cancer tissue. The test
(approved by the FDA) is useful in predicting time to
distant metastasis in women who are under age 61 who have
tumor size equal to or less than five centimeters and no
evidence that the cancer has spread to lymph nodes (lymph
node negative) (15-17).
Recently a study that compared
different prediction tests based on molecular
characteristics found that there is high concordance between
Mammaprint and Oncotype DX (18).
Breast cancer usually sends
metastasis first to regional lymph nodes. Lymph nodes of the
axilla (underarm) are usually the first to be affected;
other regional lymph nodes affected by breast metastasis are
the supraclavicular lymph nodes, infraclavicular lymph
nodes, and internal mammary lymph nodes. Distant lymph nodes
may be involved but it's rare to find distant lymph node
metastasis without regional lymph node involvement. Breast
cancer may send metastasis to every organ, but the most
involved tissues are the bones, lungs, liver and brain.
Lobular
Carcinoma in situ (LCIS).
LCIS is a premalignant state,
women with LCIS are at higher (and equal) risk to develop
breast cancer in both breasts (19) and thus local treatment
(partial resection of the breast or resection of one breast)
are not advised. Women with LCIS should be followed closely
to allow the detection of any breast malignancy at an early
stage. Preventive treatments include bilateral mastectomy
(resection of both breasts) with or without breast
reconstruction, or hormonal therapy with tamoxifen (20, 21).
Ductal
Carcinoma in situ (DCIS).
Surgery is an important arm in the treatment of DCIS. For
women suffering from DCIS, with disease limited to a part of
the breast (according to preoperative assessment e.g.
mammography), partial breast resection (lumpectomy) or total
breast resection (mastectomy) should be performed. If DCIS
lesions are scattered in different areas of the breast,
lumpectomy may turn to be impossible, and total breast
removal should be performed (mastectomy). If the resection
margins after lumpectomy contain DCIS, re-lumpectomy or
mastectomy should be performed. After lumpectomy, radiation
therapy should be delivered to the breast remnant tissue,
and this measure decreases the possibility of recurrence by
50% (22, 23). Axillary lymph node dissection is not
necessary in women with pure DCIS. For patients with a DCIS
that stains positive for estrogen receptor or progesterone
receptor, treatment with tamoxifen for 5 years is
recommended as a preventive treatment after operation.
Invasive
Cancer. Treatment of invasive
breast cancer relies on three different arms:
1)
Surgery. Surgery is used for
localized breast cancer (non metastatic disease localized to
the breast ± underarm (axillary) lymph nodes). Resection of
breast cancer is the most important part in the treatment of
localized disease. For small tumors, partial breast
resection (lumpectomy) can be satisfactory when complemented
by radiation therapy (24, 25). For large breast tumors, or
tumors involving the breast skin or nipple, resection of the
whole breast may be inevitable. In selected cases, women
with large breast tumor (without skin involvement) who
desire breast preservation may benefit from neo-adjuvant
chemotherapy, administered before the operation to shrink
the tumor size, allowing partial breast resection with good
cosmetic results (26, 27).
Determination of metastatic
disease to regional lymph nodes is preferably performed
using sentinel lymph node biopsy: in this method a dye or a
radioactive material is injected to the tumor bed (tissue
surrounding the tumor) and after 10-50 minutes the surgeon
tracks the lymph nodes to which the dye or the radioactive
material drained, and excise them. The sentinel lymph node/s
are then examined under the microscope, if tumor metastasis
is found in the sentinel lymph nodes, then a full dissection
of the axillary lymph nodes is performed. This methods spare
the patient an unnecessary lymph node dissection when the
sentinel lymph node is negative (less side effects like arm
swelling) (28, 29)
2)
Radiation therapy. There are
several clinical settings in which radiation therapy is
used:
-
Lumpectomy:
radiation therapy should be given after lumpectomy
(partial breast resection) as preventive measure.
Radiotherapy should be given after the completion of
postoperative chemotherapy. For patients without
regional lymph nodes metastasis, only the breast is
treated with radiation. In the cases of lymph node
involvement, both the breast and the regional lymph
nodes should be treated with radiotherapy (24, 25).
-
Mastectomy:
radiation therapy is given after mastectomy if lymph
nodes are involved or if the tumor diameter is larger
than 5 cm. For lymph node positive patients, both the
chest wall and the regional lymph nodes are irradiated
(30).
3)
Drugs
therapy. Drug therapies in
breast cancer are divided into 3 main categories:
Chemotherapy, hormonal therapy and biologic therapies.
-
Chemotherapy.
Chemotherapy is used in breast cancer in three main
settings:
-
Neoadjuvant
treatment: Chemotherapy
given before breast cancer operation due to large
tumors, to allow better resection and/or breast
conservation (partial resection instead of mastectomy).
Neoadjuvant chemotherapy does not give survival
advantage upon adjuvant chemotherapy (26, 27).
-
Adjuvant
chemotherapy: Adjuvant
chemotherapy is given after curative breast operation
(lumpectomy or mastectomy ± axillary lymph node
dissection) in order to eliminate microscopic tumor
focuses and to decrease the probability of breast cancer
recurrence. Adjuvant chemotherapy is usually given to
women with primary breast tumors larger than 1 cm and/or
women with node positive breast cancer (axillary lymph
nodes with tumor metastasis). For women without lymph
node involvement, tumors larger than 1 cm but less than
5 cm, positive estrogen receptors and negative HER2
receptors, further evaluation of the need of
chemotherapy can be performed using molecular
characterization of the tumor with tests such Oncotype
DX or Mammaprint. These tests evaluate the risk of
breast cancer recurrence, and the possible impact of
chemotherapy treatment on the specific patient. A
discussion between the clinician and the patient is
usually necessary before ordering these tests and after
receiving the results, in order to make a rational
treatment plan. Anthracyclines are drugs that inhibit an
enzyme in the cells called topoisomerase 2; these drugs
play a pivotal role in the treatment of breast cancer.
Doxorubicin (Adriamycin) and Epirubicin are the main
anthracyclines used in the treatment of breast cancer in
the adjuvant setting, and are given usually in
combination with other chemotherapeutic drugs (e.g.
Cyclophosphamide (Cytoxan). Anthracycline-based
polychemotherapy reduces the annual breast cancer death
rate by about 38% for women younger than 50 years of age
when diagnosed and by about 20% for those of age 50—69
years when diagnosed, largely irrespective of the use of
tamoxifen and of oestrogen receptor (ER) status, nodal
status, or other tumour characteristics (31). Such
regimens are significantly more effective than the non
Anthracycline containing regimen named CMF chemotherapy
(31).
Some of the famous combination
chemotherapy protocol:
a.
AC:
Adriamycin (doxorubicin) + Cyclophosphamide given once
every 3 weeks x 4 cycles (32, 33).
b.
AC→T:
[Adriamycin (doxorubicin) + Cyclophosphamide] every 21
days for 4 cycles → Taxol (paclitaxel)
every 21 days x 4 cycles (34).
c.
AC→T
(dose dense): [Adriamycin (doxorubicin) +
Cyclophosphamide] every 14 days for 4 cycles → Taxol (paclitaxel)
every 14 days x 4 cycles (every treatment is followed by
GCSF support, e.g. Filgrestim) (35)
d.
AC→T:
[Adriamycin (doxorubicin) + Cyclophosphamide] every 21
days for 4 cycles → Taxol (paclitaxel)
every 7 days x 12 cycles (36).
e.
TAC: [Docetaxel
(Taxotere) + Adriamycin (doxorubicin) + Cyclophosphamide]
every 21 days x 6 cycles (37).
f.
TC: [Docetaxel
(Taxotere) + Cyclophosphamide] every 21 days x 4 cycles
(38).
g.
CMF:
Cyclophosphamide + 5FU+ Methotrexate (different
schedules for administration and cycles timing) (39).
For HER 2 positive patients
see protocols including the biological therapies- below.
-
Chemotherapy
for advanced metastatic disease:
chemotherapy in this case is given to decrease tumor
size, palliate symptoms resulting from the tumor masses,
and to increase overall survival of patients. As the
goal of these treatments is palliative, highly
aggressive chemotherapeutic protocols are not widely
used. Some of the treatment options used:
a.
AC: Adriamycin
(doxorubicin) + Cyclophosphamide given once every 3 weeks x
4 cycles (32, 33).
b.
Single agent
Doxorubicin (Adriamycin).
c.
Single agent
pegylated liposomal doxorubicin (Doxil/ Caelyx) (40).
d.
Single agent
Paclitaxel (Taxol) (41).
e.
Single agent
Docetaxel (Taxotere) (42).
f.
Single agent
Capecitabine (Xeloda).
g.
Single agent
Gemcitabine (Gemzar).
h.
Single agent
Vinorelbine (Navelbine).
-
Hormonal therapy.
Pathology reports of breast cancer biopsies and the
pathology reports after breast surgery (lumpectomy or
mastectomy) should include a description of the estrogen
receptor (ER) and progesterone receptor (PR) status of
the tumor. For patients with positive ER and/or PR
expression, hormonal therapy is usually utilized as part
of the treatment plan. The main three hormonal treatment
modalities are:
A.
Tamoxifen.
Tamoxifen is used to treat both pre-menopausal and
post-menopausal women suffering from breast cancer, both in
the adjuvant and metastatic setting.
B.
Aromatase
Inhibitors. Aromatase inhibitors are not active in
premenopausal women. In postmenopausal women aromatase
inhibitors are effective in ER positive patients.
C.
LHRH
agonists/ovarian ablation.
Luteinizing-hormone releasing hormone (LHRH) is a
hormone produced by the hypothalamus, and is responsible for
the release of the hormones FSH and LH from the pituitary.
This release happens when there is a pulsatile secretion of
LHRH. LHRH agonists that have long half life results in
suppression of the release of LH and FSH, and hence ovarian
suppression.
-
Adjuvant Hormonal Therapy.
i.
Tamoxifen. For
ER-positive disease, allocation to about 5 years of adjuvant
tamoxifen reduces the annual breast cancer death rate by 31%
irrespective of the use of chemotherapy and of age (31). 5
years is significantly more effective than just 1—2 years of
tamoxifen (31).
ii.
Aromatase
Inhibitors.
a.
Aromatase
inhibitors after 2-3 years of tamoxifen:
a) Exemestane:
Intergroup Exemestane Study showed that a switch to
exemestane after 2-3 years of tamoxifen improves disease
free survival (reduce recurrence of disease), and modestly
improve patients overall survival (43).
b) Anastrozole:
Patients treated with tamoxifen for 2 years as
adjuvant therapy are less likely to experience a recurrence
of breast cancer and have improved overall survival if
they switch to anastrozole compared with
continuing tamoxifen for five years (44).
c) Letrozole:
sequential treatment with letrozole after 2 years of
tamoxifen, as compared with letrozole monotherapy,
did not improve disease-free survival. There was
no difference in overall survival between women treated with
5 years tamoxifen or 5 years letrozole (45).
b.
Aromatase
inhibitors after 5 years of tamoxifen: Treatment with
Letrozole after 5 year tamoxifen improves disease free
survival (decrease the recurrence rate of the disease) but
do not improve the patients' survival, except if lymph nodes
were involved at presentation. The ideal period of letrozole
treatment is not known, but should not exceed 2-5 years
(46).
-
Hormonal Therapy for Metastatic
Disease.
Hormonal therapies for
metastatic disease includes: Aromatase inhibitors for
postmenopausal women (preferred), Tamoxifen, LHRH ±
tamoxifen/ aromatase inhibitor (for premenopausal women),
and Fulvestrant.
-
Biologic therapies.
a)
Trastusumab (Herceptin).
Human epidermal growth factor
receptor 2 (HER 2) is found on the cell surface of 20 to
30% of invasive breast carcinomas (47). Patients with
tumors over-expressing HER2 may benefit from drugs that are
targeted to this receptor. Trastusumab is a humanized
antibody that targets the HER2 receptor. Tumor cells
over-expressing HER2 are attacked by Trastuzumab, ultimately
leading to less tumor proliferation. In the adjuvant
setting, Trastuzumab combined with paclitaxel after
doxorubicin and cyclophosphamide improves
outcomes among women with surgically removed
HER2-positive breast cancer (48, 49). The most used
treatment regimen is AC→T+H:
[Adriamycin (doxorubicin) + Cyclophosphamide] every 21 days
for 4 cycles → Taxol (paclitaxel)
every 21 days x 4 cycles + Trastuzumab (Herceptin) every 21
days for 1 year. Trastuzumab in combination with other
chemotherapies was also reported in the adjuvant setting
(50). Women with
metastatic breast cancer over-expressing HER2 also benefit
when Herceptin is added to chemotherapy (51), hormonal
therapy (52) or when given as a single agent (53). Recently,
a report showed a benefit for continuing Herceptin, in women
previously treated with Herceptin and progressed, together
with chemotherapy. The effect on overall survival was not
statistically significant, but overall response rates were
more pronounced when Heceptin was continued beyond
progression (54).
b)
Lapatinib.
Lapatinib (Tykerb) is a medication
given as an oral pill; it is a small molecule that is
absorbed through the gastrointestinal track, and arrives to
all body organs including the brain (as opposed to Herceptin
which do not penetrate the blood-brain brier). Lapatinib
inhibit the HER2 receptor through inhibiting its
intracellular (tyrosine kinase) part. Lapatinib when added
to capecitabine is superior to capecitabine alone
in women with HER2-positive advanced breast cancer that
has progressed after treatment with regimens that
included an anthracycline, a taxane, and
trastuzumab (55). Recent report by Kaufman et al. showed
that Lapatinib monotherapy is a potentially effective
treatment for relapsed or refractory HER2+ inflammatory
breast cancer (56).
c)
Bevacizumab (Avastin).
Bevacizumab is a
monoclonal antibody against VEGF. Initial therapy of
metastatic breast cancer with bevacizumab plus
paclitaxel as compared with paclitaxel alone, increases the
objective response rate but do
not prolong overall survival or
improve quality of life (57). Adding Avastin to capecitabine
in treatment of women with metastatic breast cancer didn't
resulted in prolongation of life of these patients, nor
resulted in slowing of the disease progression (58).
-
Jemal A. et al. Cancer statistics, 2009. CA Cancer J Clin.
59:225-249 (2009).
To read this article press here.
-
WHO World Cancer Report, World Health Organization, (2003).
-
McArthur HL, Hudis CA. Has first-line therapy had an impact on
general outcome in metastatic breast cancer? Future
Oncol. 2007; 3(4):411-8.
To read this article press here.
-
El Saghir NS, Khalil MK, Eid T, El Kinge AR, Charafeddine M,
Geara F, Seoud M, Shamseddine AI. Trends in epidemiology
and management of breast cancer in developing Arab
countries: a literature and registry analysis. Int J
Surg. 2007; 5(4):225-33.
To read this article press here.
-
Ziedan J. et al. Clinical And Pathological Features Of Breast
Cancer In Arab Compared To Jewish Women At The Galilee
Area. ISCORT, Eilat, 2009.
To read this abstract press here.
-
DeVita VT, Laurance TS, Rosenberg SA. Cancer principles &
practice of oncology. 8th Edition.
Lippincott, Williams & Wilkins., USA, 2008.
www.LWW.com.
-
Tryggvadóttir L, Tulinius H, Eyfjord JE,
Sigurvinsson T. Breastfeeding and reduced risk of breast
cancer in an Icelandic cohort study. Am J Epidemiol.
154(1):37-42 (2001).
To read this article press here.
-
Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ.
Overweight, obesity, and mortality from cancer in a
prospectively studied cohort of U.S. adults. N Engl J
Med. 348(17):1625-38 (2003).To
read this article press here.
-
Thune I, Brenn
T, Lund E, Gaard M.
Physical activity and the risk of breast
cancer. N Engl J Med. 336(18):1269-75 (1997).
To read this article press here.
-
American Joint Committee on Cancer, cancer staging
manual 6th edition, NY, Springer –Verlag,
2002.
-
www.oncotypedx.com (2009)
-
Paik S, et al.
A Multigene Assay to Predict Recurrence of Tamoxifen-Treated,
Node-Negative Breast Cancer. N Engl J Med. 351:
2817-2826 (2004).
To read this article press here.
-
Paik S, et al.
Gene Expression and Benefit of Chemotherapy in Women
with Node-Negative, Estrogen Receptor-Positive Breast
Cancer. J Clin Oncol. 24(23):3726-3734 (2006).
To read this article press here.
-
Goldstein LJ. et al. Prognostic Utility of
21-Gene Assay in Hormone Receptor (HR) Positive Operable
Breast Cancer and 0-3 Positive Axillary Nodes Treated
with Adjuvant Chemohormonal Therapy (CHT): An Analysis
of Intergroup Trial E2197. ASCO (2007).
To read this abstract press here.
-
Van 't Veer LJ. et al.
Gene expression profiling predicts clinical outcome
of breast cancer.
Nature
415, 530-536 (2002).
To read this article press here.
-
Van de Vijver MJ. Et al. A Gene-Expression
Signature as a Predictor of Survival in Breast Cancer. N
Engl J Med. 347: 1999-2009 (2002).
To read this article press here.
-
FDA Clears Breast Cancer Specific Molecular
Prognostic Test.
FDA web site.
-
Fans C. et al. Concordance among
Gene-Expression–Based Predictors for Breast Cancer. N
Engl J Med. 355:560-569 (2006).
To read this article press here.
-
Chuba PJ. et al. Bilateral Risk for
Subsequent Breast Cancer After Lobular
Carcinoma-In-Situ: Analysis of Surveillance,
Epidemiology, and End Results Data. J Clin Oncol. 23:
5534-5541 (2005).
To read this article press here.
-
Fischer B. et al. Tamoxifen for the Prevention of Breast
Cancer: Current Status of the National Surgical Adjuvant
Breast and Bowel Project P-1 Study. J Natl Cancer Inst.
901371-88 (1998).
To read this article press here.
-
Fischer B. et al. Tamoxifen for the prevention of breast
cancer: current status of the National Surgical Adjuvant
Breast and Bowel Project P-1 study. J Natl Cancer Inst.
97(22):1652-62 (2005).
To read this article press here.
-
Bijker N. et al. Breast-Conserving
Treatment With or Without Radiotherapy in Ductal
Carcinoma-In-Situ: Ten-Year Results of European
Organisation for Research and Treatment of Cancer
Randomized Phase III Trial 10853—A Study by the EORTC
Breast Cancer Cooperative Group and EORTC Radiotherapy
Group. J Clin Oncol, 24: 3381-3387 (2006).
To
read this article press here.
-
Fisher B. et al. Lumpectomy and radiation
therapy for the treatment of intraductal breast cancer:
findings from National Surgical Adjuvant Breast and
Bowel Project B-17. J Clin Oncol, 16: 441-452 (1998).
To read this article press here.
-
Veronesi U. et al. Twenty-Year Follow-up of
a Randomized Study Comparing Breast-Conserving Surgery
with Radical Mastectomy for Early Breast Cancer. N Engl
J Med. 347:1227-1232 (2002).
To read this article press here.
-
Fisher B. et al. Twenty-Year Follow-up of a
Randomized Trial Comparing Total Mastectomy, Lumpectomy,
and Lumpectomy plus Irradiation for the Treatment of
Invasive Breast Cancer. 347:1233-1241 (2002).
To read this article press here.
-
Fisher B. et al. Effect of preoperative
chemotherapy on the outcome of women with operable
breast cancer. J Clin Oncol. 16: 2672-2685 (1998).
To read this article press here.
-
Bear HD. et al. Sequential preoperative or
postoperative docetaxel added to preoperative
doxorubicin plus cyclophosphamide for operable breast
cancer: national surgical adjuvant breast and bowel
project protocol B-27. J Clin Oncol. 24: 2019-2027
(2006).
To read this article press here.
-
Veronesi U. et al. A randomized comparison
of sentinel lymph node biopsy with routine axillary
dissection in breast cancer. N Engl J Med. 349: 546-553
(2003).
To read this article press here.
-
Mansel RE. et al. Randomized multicenter
trial of sentinel node biopsy versus standard axillary
treatment in operable breast cancer: The ALMANAC trial.
J Natl Cancer
Inst. 98: 599-609 (2006).
To read this article press here.
-
Overgaard M. et al. Postoperative
radiotherapy in high-risk premenopausal women with
breast cancer who receive adjuvant chemotherapy. N Engl
J Med. 337: 949-955 (1997).
To read this article press here.
-
Early Breast Cancer Trialists'
Collaborative Group. Effects of chemotherapy and
hormonal therapy for early breast cancer on recurrence
and 15-year survival: an overview of the randomised
trials. The Lancet, 365: 1687-1717 (2005).
-
Fisher b. et al.
Two months of doxorubicin-cyclophosphamide with
and without interval reinduction therapy compared with 6
months of cyclophosphamide, methotrexate, and
fluorouracil in positive-node breast cancer patients
with tamoxifen-nonresponsive tumors: results from the
National Surgical Adjuvant Breast and Bowel Project
B-15. J Clin Oncol. 8: 1483-1496 (1990).
To read this article press here.
-
Fisher b. et al. Postoperative chemotherapy
and tamoxifen compared with tamoxifen alone in the
treatment of positive-node breast cancer patients aged
50 years and older with tumors responsive to tamoxifen:
results from the National Surgical Adjuvant Breast and
Bowel Project B-16. J Clin Oncol. 8: 1005-1018
(1990).
To read this article press here.
-
Mamounas EP. et al. Paclitaxel After
Doxorubicin Plus Cyclophosphamide As Adjuvant
Chemotherapy for Node-Positive Breast Cancer: Results
From NSABP B-28. J Clin Oncol. 23: 3686-3696 (2005).
To read this article press here.
-
Citron
ML. et al. Randomized Trial of Dose-Dense Versus
Conventionally Scheduled and Sequential Versus
Concurrent Combination Chemotherapy as Postoperative
Adjuvant Treatment of Node-Positive Primary Breast
Cancer: First Report of Intergroup Trial C9741/Cancer
and Leukemia Group B Trial 9741. J Clin Oncol. 21:
1431-1439.
To read this article press here.
-
Sparano JA. et al.
Weekly Paclitaxel in the Adjuvant Treatment
of Breast Cancer. N Engl J Med. 358:1663-1671 (2008).
To read this article press here.
-
Martin M. et al. Adjuvant Docetaxel for
Node-Positive Breast Cancer. N Engl J Med. 352:2302-2313
(2005).
To read this article press here.
-
Jones SE. Phase III Trial Comparing
Doxorubicin Plus Cyclophosphamide With Docetaxel Plus
Cyclophosphamide As Adjuvant Therapy for Operable Breast
Cancer. J Clin Oncol. 24: 5381-5387 (2006).
To read this article press here.
-
Colleoni GM. Adding adjuvant CMF
chemotherapy to either radiotherapy or tamoxifen: Are
all CMFs alike? Ann Oncol 9: 489-493.
To read this article press here.
-
O'Brien ME. Single-agent treatment with pegylated liposomal
doxorubicin for metastatic breast cancer. Anticancer
Drugs 19:1-7 (2008).
To read this article press here.
-
Miller k. et al. Paclitaxel plus
Bevacizumab versus Paclitaxel Alone for Metastatic
Breast Cancer. N Engl J Med. 357:2666-2676 (2007).
To read this article press here.
-
Jones SE. et al. Randomized Phase III Study
of Docetaxel Compared With Paclitaxel in Metastatic
Breast Cancer. To read this article press here. J Clin
Oncol. 23: 5542-5551 (2005).
To read this article press here.
-
Coombes RC. et al. Survival and safety of
exemestane versus tamoxifen after 2—3 years' tamoxifen
treatment (Intergroup Exemestane Study): a randomised
controlled trial. Lancet 369: 559-570 (2007).
To read this article press here.
-
Kaufman M. et al. Improved Overall Survival
in Postmenopausal Women With Early Breast Cancer After
Anastrozole Initiated After Treatment With Tamoxifen
Compared With Continued Tamoxifen: The ARNO 95 Study. J
Clin Oncol. 25: 2664-2670 (2007).
To read this article press here.
-
The BIG 1-98 Collaborative Group. Letrozole
Therapy Alone or in Sequence with Tamoxifen in Women
with Breast Cancer. N Engl J Med. 361: 766-776 (2009).
To read this article press here.
-
Goss PE. et al. Randomized Trial of
Letrozole Following Tamoxifen as Extended Adjuvant
Therapy in Receptor-Positive Breast Cancer: Updated
Findings from NCIC CTG MA.17. JNCI 97: 1262-1271 (2005).
To read this article press here.
-
Hudis CA. Trastuzumab — Mechanism of Action
and Use in Clinical Practice. N Engl J Med. 357:39-51
(2007).
To read this article press here.
-
Romond EH. et al. Trastuzumab plus Adjuvant
Chemotherapy for Operable HER2-Positive Breast Cancer. N
Engl J Med. 353:1673-1684 (2005).
To read this article press here.
-
Piccart-Gebhart MJ. et al. Trastuzumab
after Adjuvant Chemotherapy in HER2-Positive Breast
Cancer. N Engl J Med. 353: 1659-1672 (2005).
To read this article press here.
-
Joensuu H. et al.
Adjuvant Docetaxel or Vinorelbine with or
without Trastuzumab for Breast Cancer. N Engl J Med.
354:809-820 (2006).
To read this article press here.
-
Slamon DJ. Use of Chemotherapy plus a
Monoclonal Antibody against HER2 for Metastatic Breast
Cancer That Overexpresses HER2. 344:783-792 (2001).
To read this article press here.
-
Kaufman B. Trastuzumab Plus Anastrozole
Versus Anastrozole Alone for the Treatment of
Postmenopausal Women With Human Epidermal Growth Factor
Receptor 2–Positive, Hormone Receptor–Positive
Metastatic Breast Cancer: Results From the Randomized
Phase III TAnDEM Study. J Clin Oncol. 27: 5529-5537
(2009).
To read this article press here.
-
Vogel CL. Efficacy and Safety of
Trastuzumab as a Single Agent in First-Line Treatment of
HER2-Overexpressing Metastatic Breast Cancer. J
Clin Oncol. 20: 719-726 (2002).
To read this article press here.
-
Von Minckwitz G. Trastuzumab Beyond
Progression in Human Epidermal Growth Factor Receptor
2–Positive Advanced Breast Cancer: A German Breast Group
26/Breast International Group 03-05 Study. J Clin Oncol.
27: 1999-2006 (2009).
To read this article press here.
-
Geyer CE. et al. Lapatinib plus
Capecitabine for HER2-Positive Advanced Breast Cancer.
N Engl J Med.
355:2733-2743 (2006).
To read this article press here.
-
Kaufman B. et al. Lapatinib monotherapy in
patients with HER2-overexpressing relapsed or refractory
inflammatory breast cancer: final results and survival
of the expanded HER2+ cohort in EGF103009, a phase II
study. Lancet Oncology. 10: 581-588 (2009).
To read this article press here.
-
Miller K. et al. Paclitaxel plus Bevacizumab versus Paclitaxel Alone for
Metastatic Breast Cancer. N Engl J Med. 357:2666-2676
(2007).
To read this article press here.
-
Miller K. et al. Randomized Phase III Trial of
Capecitabine Compared With Bevacizumab Plus Capecitabine
in Patients With Previously Treated Metastatic Breast
Cancer.
J Clin Oncol. 23: 792-799 (2005).
Press here to view the article abstract.
|